Patient Outreach Agent - Design Time Experience
A nurse knows how to talk to patients. Designing the experience that teaches an AI agent to do it on their behalf.
Context: Before procedures, nurses call patients to collect medical history, screen for risks, and provide preparation instructions. These calls follow structured questionnaires — the same questions, in roughly the same order, for every patient. Patient Outreach Agent automates these calls: the AI agent calls the patient, conducts the conversation, and populates the form for the nurse's review. Pre-Anesthesia Screening is used as the illustrative example throughout — actual form structure varies by clinical use case and institution.
At a Glance
< 45 minutes to author an outreach agent
Scenario coverage
5–10x increase in scenario coverage before publish
The Problem
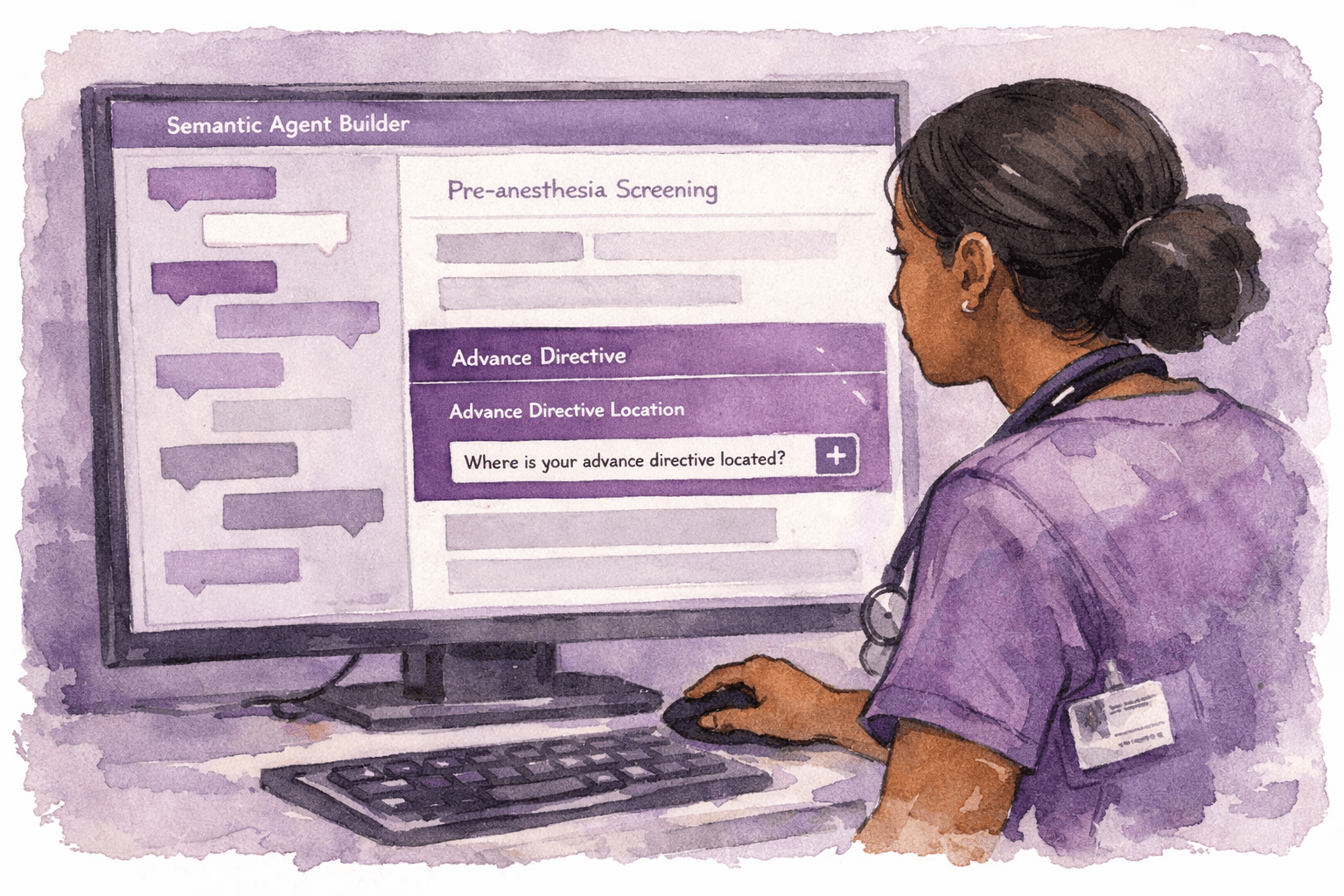
Patient outreach calls are time-consuming, repetitive, and pull nurses away from direct patient care. The agent can make the call — but only if it knows how to ask each question the way a skilled nurse would. A form field labeled "Height" produces an agent that says "Height" to a patient. That's not a conversation. Teaching the agent to ask "What is your height?" — and hundreds of questions like it — is what this design-time experience enables.
My Role
Product thinking lead: No dedicated PM
Cross-functional: PM, engineering, data science
The Solution
An informaticist or nurse opens a patient outreach form in SAB. The form structure loads on the Canvas — every section and field visible, each with a quote icon (to add a verbalized question — the human-language phrasing the agent will use when asking) and an eye icon (to show or hide the field from the agent's conversation). They choose how to add verbalized questions: upload a PDF document and SAB maps questions to fields automatically, or work through the form field by field — either by tapping the quote icon on the canvas or letting the SAB agent guide them conversationally.

Key Design Decisions
From "adjust the knobs" to verbalized questions
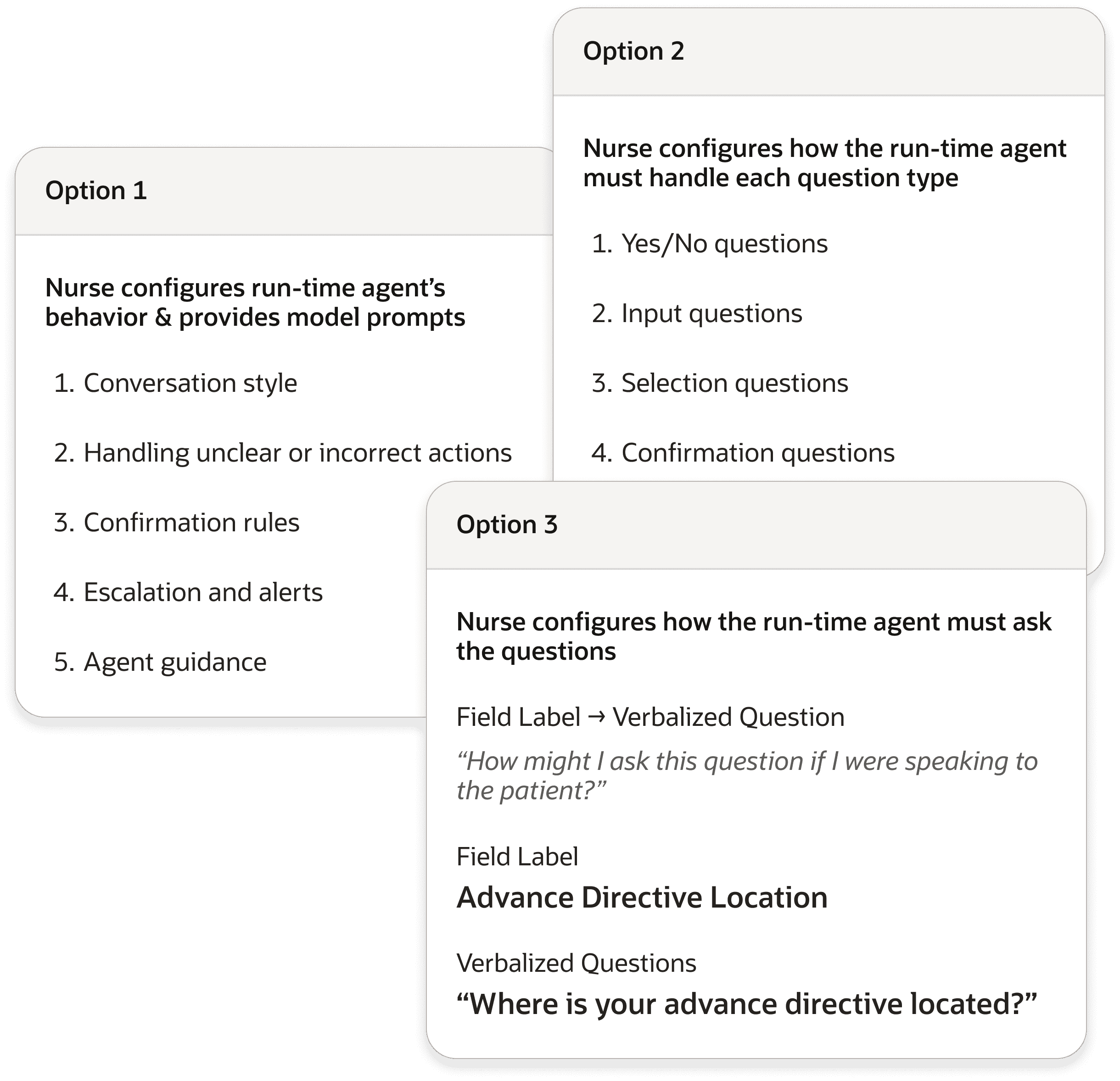
Initial requirements were undefined — the ask was for SAB to add "metadata" and let nurses "adjust knobs." Nobody could define what these meant. I used AI tools to research patient outreach workflows clinically, proposed 3 competing design directions, and presented them to the cross-functional team simultaneously. That presentation made the unresolved questions undeniable. The data science team finally gave specific signal: the agent needed human language attached to every form field. Not the field label — a real question, phrased the way a nurse would actually say it to a patient.
Two ways to teach the agent
Nurses with an existing document of verbalized questions can upload it — SAB maps questions to fields and proactively flags unmatched ones, asking whether to add questions manually or skip those fields. Nurses who prefer to work field by field can tap a quote icon directly on the canvas, or let the SAB agent walk them through section by section conversationally. Both paths produce the same output. The nurse chooses how to get there.

Show/hide: nurse controls what the agent covers
An eye icon on every section and field. Visible means the agent asks it. Hidden means it skips it. Simple, scannable, consistent. Fields without a verbalized question must be hidden before the agent can run — SAB surfaces this proactively, before it becomes a runtime failure.

Impact
The 5 conversation configuration dimensions I proposed proactively — conversation style, confirmation rules, escalation logic, handling of unclear answers, and section-specific agent guidance — went beyond what anyone asked for. The team is now actively considering building them into future phases.
What's Next
Phase 1 — verbalized questions and show/hide — launches Q2 2026. With Care Pathway and Patient Outreach both in SAB, the platform now spans clinical decision support and patient communication — two fundamentally different agent types, one no-code authoring infrastructure.